Do you feel pain in your knee on climbing stairs or even squatting after your run? Feeling weird that it doesn’t hurt while you run? Then, chances are, you might be suffering from anterior knee pain. Knee pain is the most common running injury, occurring in approximately 55% of recreational runners. Of this number, 65% will have severity of symptoms that will require them to seek medical attention or contemplate cessation of running. Anterior Knee Pain (Anterior Knee Pain), otherwise known as Patellar Femoral Pain, has been found to be one of the most common condition resulting in knee pain. It has been estimated to have an incidence of 25% of all knee injuries.
In recent years, there have been a number of researches looking into preventing and managing Anterior Knee Pain (AKP) and as a result, predicting factors have also been found. In this article, we’ll be looking at the factors that would predict one’s pre-disposition to developing Anterior Knee Pain, its management and prevention.
Etiological Factors of Anterior Knee Pain
There have been many etiological factors that have been linked to Anterior Knee Pain. These factors can be broadly grouped under the following:
- Muscular faults
- Structural Faults
- Training Faults
Amongst these faults, researches have shown that the combination of the factors below have the highest co-relation in predicting the development of Anterior Knee Pain:
- Lack of pronation of the rear footon heel strike – Increases the strain that the knee undergoes due to the lackof absorption of the ground reaction force.
- Foot type (pes cavus) –Athletes with pes cavus or high arch foot type have a smaller surface area ofcontact thus increasing the ground reaction force.
- Lack of strength and/or enduranceof quadriceps – correlates with an increased impact of the knee during arun
- Increased Q angle – More pronounced in females as their pelvisesare generally wider than that of men’s. The increase in tension of the ITB inturn results in an increase in the internal rotation (turning in) of the hip. Thiscreates even more tension through the ITB. As the ITB has attachments to thelateral retinaculum, a tight ITB will pull on the patellar laterally resulting in alaterally shifted and tilted patellar. This alters the pressures under the surfaceof the patella, causing a premature wearing out of the cartilage and increasing therisk of degeneration and pain
- Training methods –training on hard surfaces and premature change of footwear had been found toincrease risk of Anterior Knee Pain.
Muscular Faults leading to Anterior Knee Pain
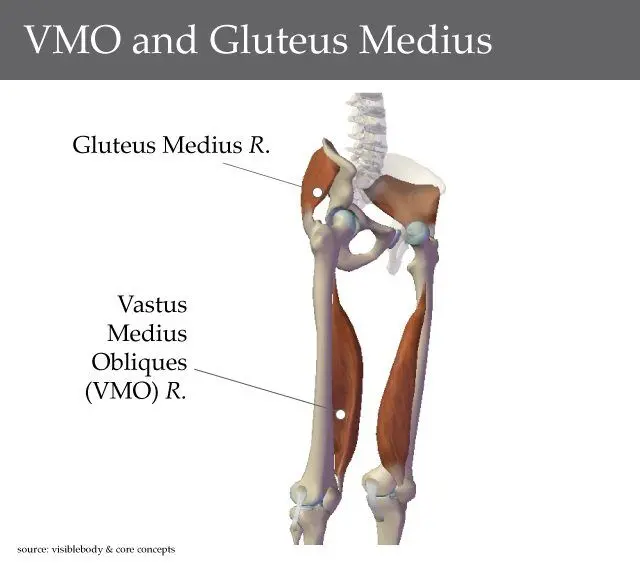
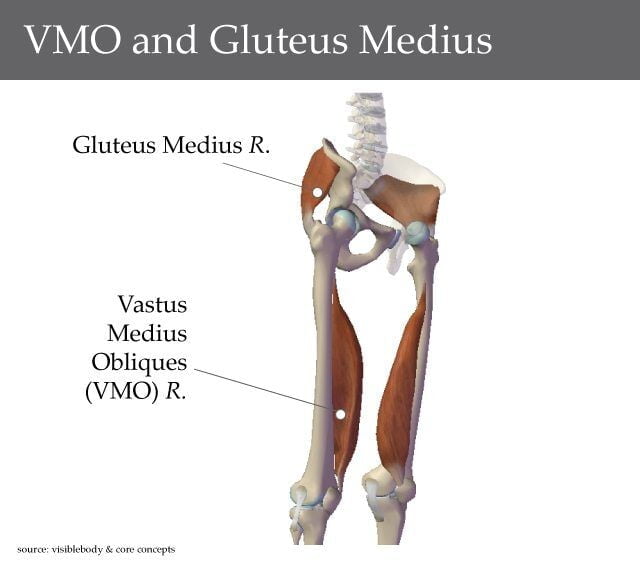 Weakness in Gluteus Medius (GM) and Vastus Medialis Obliques (VMO) muscles are the main muscular causes of Anterior Knee Pain. The primary function of Gluteus Medius is to externally rotate the hip while the VMO aids in knee extension with a secondary role in the stabilization of the patellar. These two muscles works as a sling to aid in stabilizing the hip (figure 1). Weakness, or rather the lack of motor control of the GM would lead to an internal rotation of the hip. This would, in turn, cause a tension of the ITB, which would pull the patellar laterally, affecting the length-tension relationship of the VMO. The VMO would be lengthen, thus affecting not only the activation timing but also the strength. This causes a mismatch in the force working to center the patellar within the femoral groove, leading to a possible degeneration of the cartilage behind the patellar, which might then cause pain.
Weakness in Gluteus Medius (GM) and Vastus Medialis Obliques (VMO) muscles are the main muscular causes of Anterior Knee Pain. The primary function of Gluteus Medius is to externally rotate the hip while the VMO aids in knee extension with a secondary role in the stabilization of the patellar. These two muscles works as a sling to aid in stabilizing the hip (figure 1). Weakness, or rather the lack of motor control of the GM would lead to an internal rotation of the hip. This would, in turn, cause a tension of the ITB, which would pull the patellar laterally, affecting the length-tension relationship of the VMO. The VMO would be lengthen, thus affecting not only the activation timing but also the strength. This causes a mismatch in the force working to center the patellar within the femoral groove, leading to a possible degeneration of the cartilage behind the patellar, which might then cause pain.
Although mentioned earlier that lack of pronation on heel strike predisposes athletes to Anterior Knee Pain, some studies have shown a strong correlation with over-pronation of the foot leading to AKP. It is believed that over-pronation of the foot would lead to the knee turning inwards, causing the ilio-tibial band (ITB) to be under tension, increasing the risk of mal-tracking of the patellar. Tight calf muscles, especially the soleus, have been linked to over-pronation of the foot, which would cause the knee to turn inwards.
Anterior Knee Pain Management
| Muscular Faults | Management / Prevention |
|
|
Structural Faults leading to AKP
The most common structural faults leading to Anterior Knee Pain is foot type. Both high arch feet and runners who tend to over-pronate on weight-bearing are at risk. However, research has found that athletes with a high arch foot are at greater risk of developing AKP as compared to flat or pronated feet. This has been attributed to the fact that a rigid foot with a high arch has an increased load per surface area on impact. It has also been found that those with high arch foot tend to have a stiffer rear foot thus leading to a lack of rear foot pronation on heel strike of running.
Patellar tilt, an increased Q angle and available full range of movement of the knee are also common structural faults that would lead to AKP but however, there’s only very little can be done to correct these faults.
| Structural faults | Management / Prevention |
|
|
Training Faults
Pre-matured discarding of running shoes and weekly mileage are the 2 most common training faults. Research has found that the optimal mileage on 1 pair of foot wear should be about 800–1000km. However, most runners with knee pain tend to discard their shoes after about 500-600km, due to discomfort. This point is highly contentious as most would think that once the shoe starts to wear out, one would need to change to ensure proper support. However, further research were done and support for this point attributed that frequent change of shoes increases the risk of Anterior Knee Pain as the foot would need to get re-accustomed to the support of the shoe.
There has also been a co-relation between the mileage an athlete can run pain-free and the number of etiological factors that may cause Anterior Knee Pain. This is an inverse relationship, i.e. athletes who have more etiological factors that predispose them to Anterior Knee Pain, their weekly mileage should be lower (refer to diagram 1).
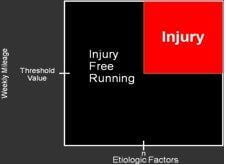 Diagram 1
Diagram 1
Other factors that can be changed to prevent or manage training faults are changing the running surfaces to softer surfaces like stadium running track surface or grass, instead of crowned, hard surfaces like the road or cemented pavements. Slow, progressive increment of running distance and speed are as important in preventing Anterior Knee Pain as proper running techniques.
Anterior Knee Pain are Preventable
In summary, knee pain in runners, though is common, is preventable through the identification of these 5 predicting etiological factors and taking the following precautions:
| Etiological Factors | Preventative Precautions |
|
|